This option of CPDMS.net contains programs for exchanging information between the statewide database and individual hospitals, and between individual hospitals and external organizations. Note that incomplete records are NOT included in files generated by the various data exchange functions.
RCRS Submission
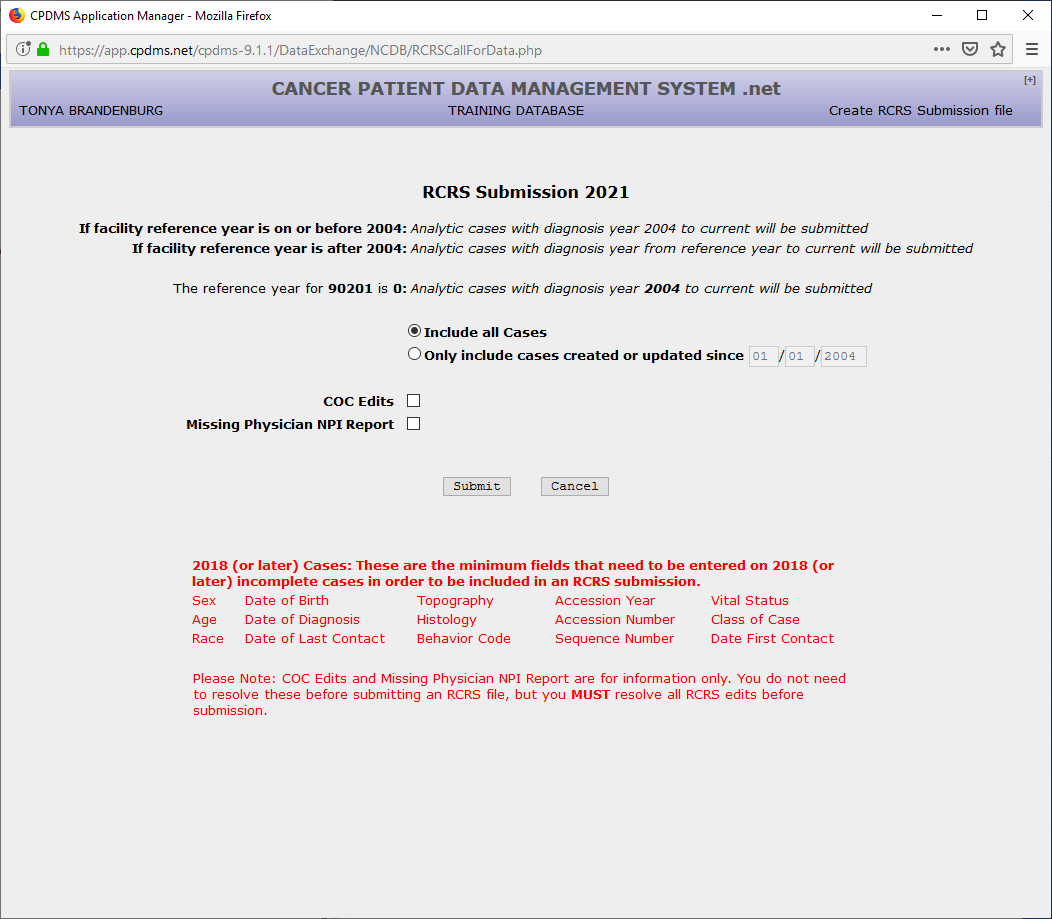
This feature of CPDMS.net allows users to create files for Rapid Cancer Reporting System. You can choose to include all cases or only cases created or updated since a certain date. Then choose if you want to review the COC edits and Missing Physician NPI Report and then click "Submit."
An example is shown below of what the beginning screen looks like:
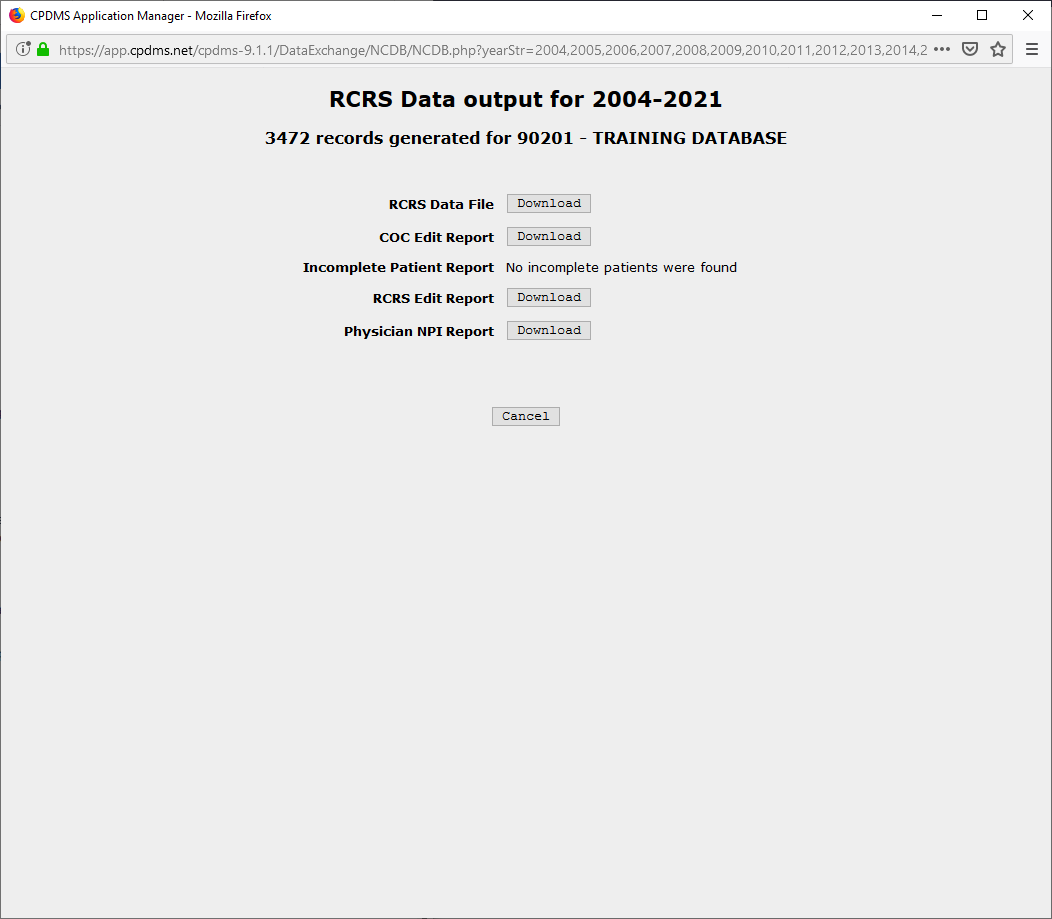
An example is shown below in which edit checks, incomplete patients, and the missing physician NPI report were all generated for all years data and are available for download.
Death Clearance
This feature of CPDMS.net allows individual Kentucky hospitals to match their patient demographic data with the state's annual death certificate listings. The Kentucky Department of Vital Statistics provides KCR with an electronic file of all death certificates filed in Kentucky each calendar year. This file is then matched with the KCR central database and an individual electronic file is created for each hospital registry in the state.
The file sent to each hospital contains the names and other identifying information of all patients in that registry who also appeared on the state death certificate list.
The list of matching names is compiled and transmitted to each hospital annually. Through this process, hospitals may identify patients in their registries who have died (due to any cause) and then update their records accordingly.
In order to perform death clearance, select "Death Clearance" from the Data Exchange menu. The following screen appears:
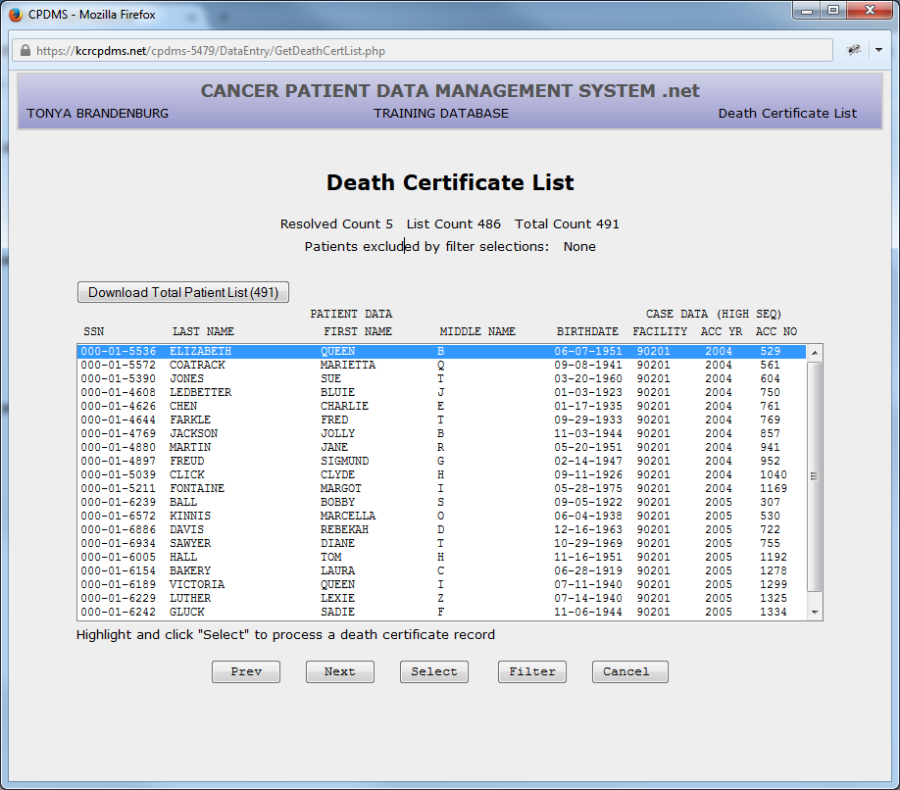
This screen contains a list of all death certificates which are probable matches to patients in a particular registry. The SSN, Last Name, First Name, Middle Name, and Birth Date from the death certificate are listed, as well as the ID number of the facility which initially created the patient. "Prev" and "Next" are used to scroll through multi-page death certificate lists, while "Cancel" returns to the Main Menu. In order to process the death certificates, highlight a record and click "Select."
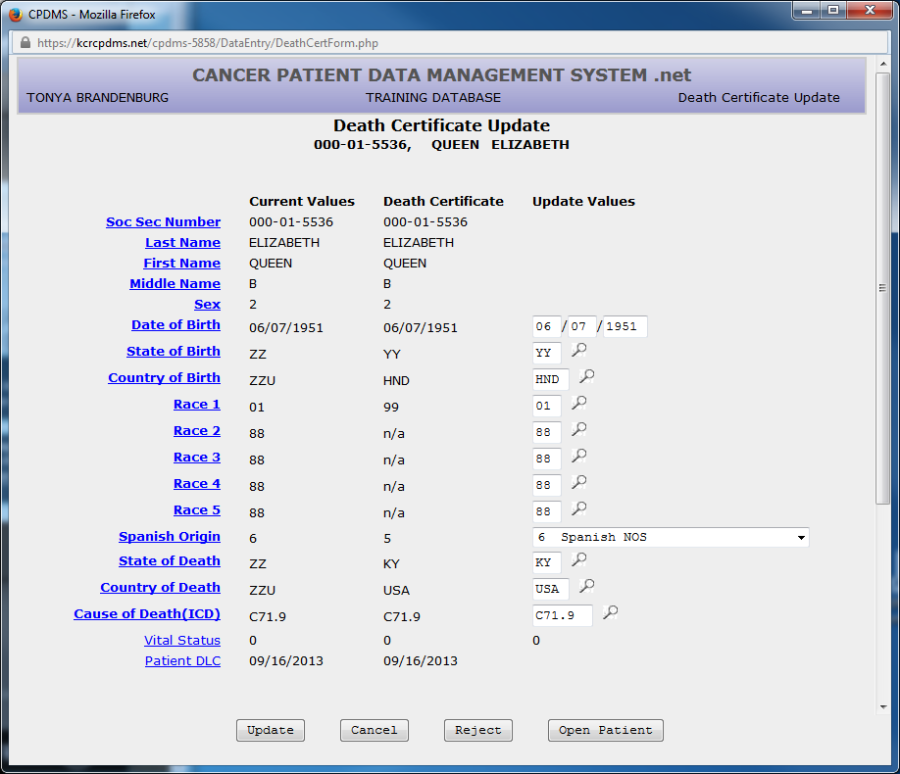
Now the death certificate record is displayed side by side with the values from the patient record.
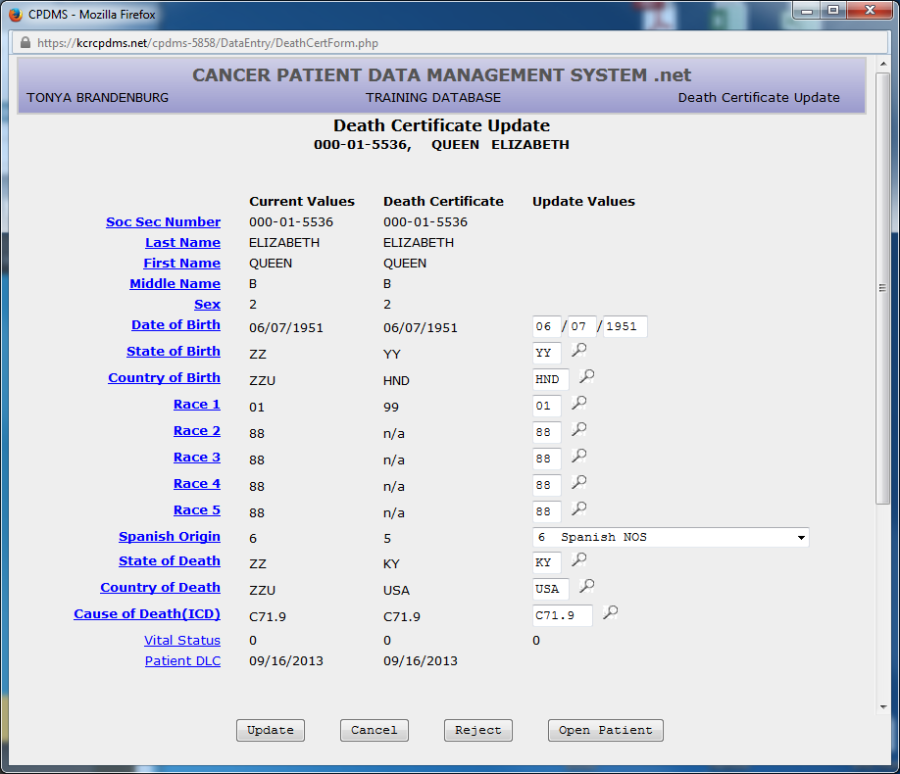
Choose "Cancel" at any time to return to the Death Certificate List without processing this record. Carefully compare the two records to determine that they are actually the same individual. If they are not, click the "Reject" button at the bottom of the screen. The following message appears:
Choose "OK" to reject the link and "Cancel" to return to the death certificate update screen.
If the death certificate record and patient record are truly a match, the patient and case follow-up values should now be updated.
The feature was recently added the gives the ability to open a patient in data entry from the death certificate update form.
Users may update the following patient level fields: Date of Birth, State of Birth, Country of Birth, Race 1-5, Spanish Origin, State of Death, Country of Death, and Cause of Death. The fields are filled in with default values, but these may be overwritten. The priority which CPDMS.net uses when assigning the defaults is as follows:
Date of Birth- always set to patient record value
State of Birth- set to the death certificate value if the patient record value is ZZ, or if the patient record value is less specific than the death certificate value
Country of Birth - set to the death certificate value if the patient record value is ZZU, or if the patient record value is less specific than the death certificate value
Race 1- set to death certificate value if patient record value is 99 or blank and death certificate value is not 99
Race 2-5- set to 88 if Race 1 is taken from the death certificate; otherwise set to the patient record value
Spanish Origin- set to death certificate value if the patient record is 9 OR if the patient record is 0 but the death certificate record is 1-8
State of Death - set to the death certificate value if the patient record value is ZZ, or if the patient record value is less specific than the death certificate value
Country of Death - set to the death certificate value if the patient record value is ZZU, or if the patient record value is less specific than the death certificate value
Cause of Death- always set to death certificate value
The calculated field Vital Status is set to zero and cannot be edited in the Death Certificate Update form. The Patient DLC is automatically set to the latest Case Follow- Up Date of Last Contact after the Death Certificate Update is saved.
NOTE: Due to the high frequency of inaccuracies in death certificate records, users are not given the option of editing SSN, Last Name, First Name, Middle Name, or Sex in this form. When these fields differ between the patient record and death certificate record, do not edit the patient record unless there is additional evidence that the death certificate record is correct. The exception to this rule is fake SSN's, which should be updated with the SSN from the death certificate. In order to update any of these fields, simply edit or key change them after escaping from this screen.
Scroll down the page to update the case follow-up record information.
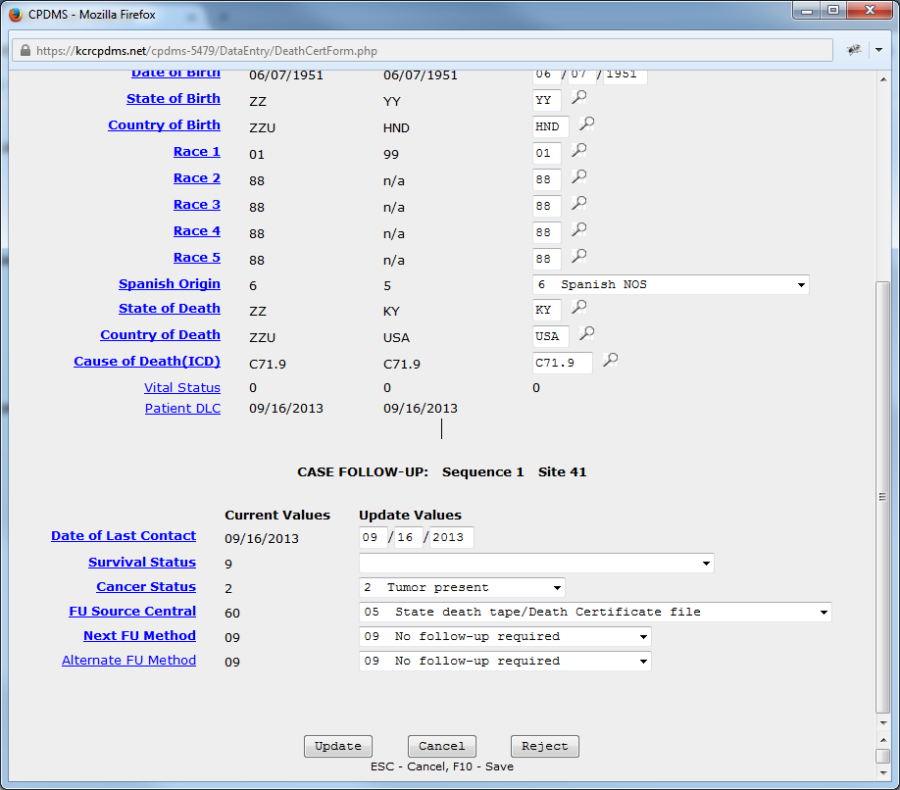
The fields Date of Last Contact, Survival Status, Cancer Status, FU Source Central, Next Follow-up Method, and Alternate Follow-up Method are available for editing. As with patient level fields, the follow-up fields are assigned default values which may be overwritten. The priority for assigning these values is as follows:
Date of Last Contact- always set to death certificate value
Survival Status- set to the value in the follow-up record if value is 4-6; set to blank if value in the follow-up record is 1-3 or 9
Cancer Status- always set to value in follow-up record
FU Source Central- always set to 05 (state death tape/death certificate file) Next and Alternate FU Methods- both always set to 09 (no follow-up required)
NOTE: If a patient has more than one case, the follow-up record for each case is available for editing in the update screen.
Once all the fields have been compared and edited, click "Update."
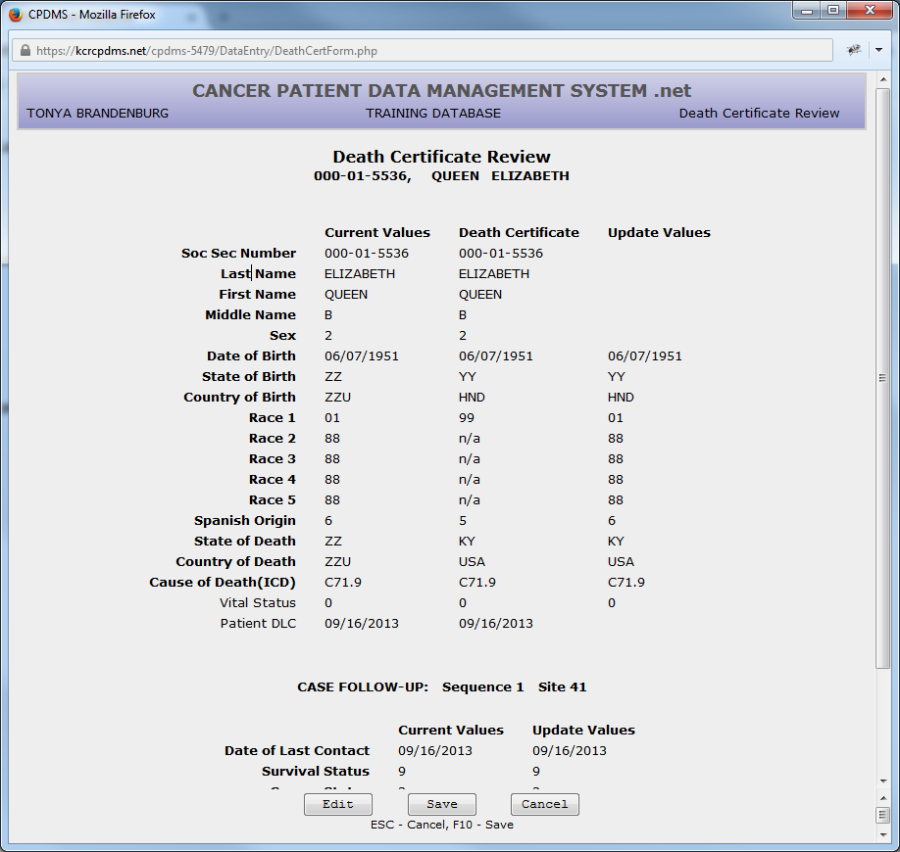
Now the fields which will be updated are shown once more and users have the opportunity to briefly review them for accuracy. Choose "Edit" to go back and change any values, "Cancel" to escape to the Death Certificate List without updating the record, or "Save" to automatically save these changes in the Patient and Case Follow-Up records. If any errors were detected by edit checks, an error message will appear. The screen will then go directly to the Data Entry Status screen, where the patient's data may be edited at that time or saved with errors.If no errors were found, the screen returns directly to the death certificate list. The death certificate which was processed no longer appears on the list.
Continue until all death certificates have been processed and the list is empty. Any death certificates which remain when a new year's group of certificates is loaded will be overwritten. If a user attempts to choose
Death Clearance from the Data Exchange menu when no death certificates are available, a message appears stating "There are no death certificates to be resolved."
Central Follow-Up
This feature allows hospitals to compare the follow-up data of their patients with that in the KCR central database. This comparison is performed monthly at the central registry, and a report is then generated for each hospital which lists the follow-up data in the central registry next to the data in the hospital registry and highlights the discrepancies. The Follow-Up report is automatically downloaded to a facility's database and users are notified via email when it is available.
Follow-up data from the central registry is listed when any of the following situations occurs: if the Date of Last Contact is later than the hospital's date, or if any of the values coded in the fields Survival Status, Type of First Recurrence, Disease Free Start Date, Date of First Recurrence, Treatment Composite First, or Treatment Composite All do not match.
In order to view the Central Follow-Up report, choose "Central Follow-Up" from the Data Exchange menu.
The screen which appears allows users to set parameters for the report. (See example below.)
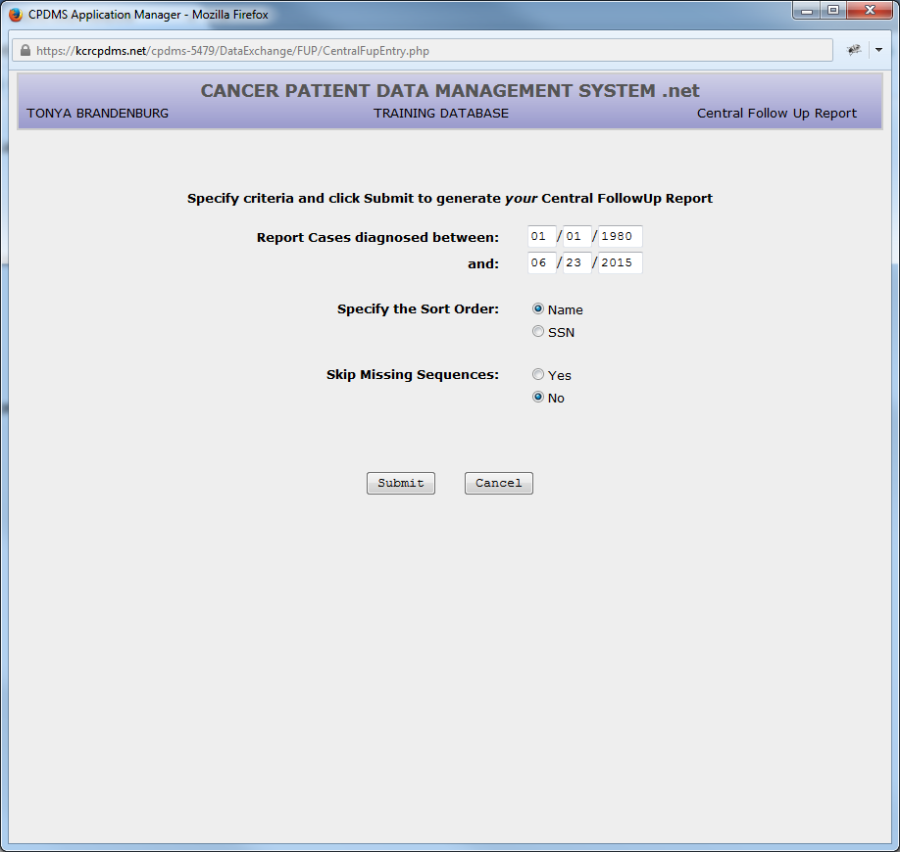
Users must specify a range of diagnosis dates for the cases to be included. The default range is 1/1/1980 to the present date, but this may be overwritten with any valid date range. The report can be sorted by either name (the default) or social security number. Subsequent primaries which were reported by other institutions can be displayed by choosing "No" for "Skip Missing Sequences." Change this to "Yes" to avoid including these. Click the 'Submit' button to generate the report.
The report is in HTML format, so it must be downloaded to a user's computer and viewed using a web browser. Click the "Download" button in order to save the report. Choose "Cancel" to return to the main menu.
After saving the Central Follow-Up report, double click to view it. The file should automatically open in a new window in Internet Explorer (note: it can be viewed in any web browser). A sample report is shown below.
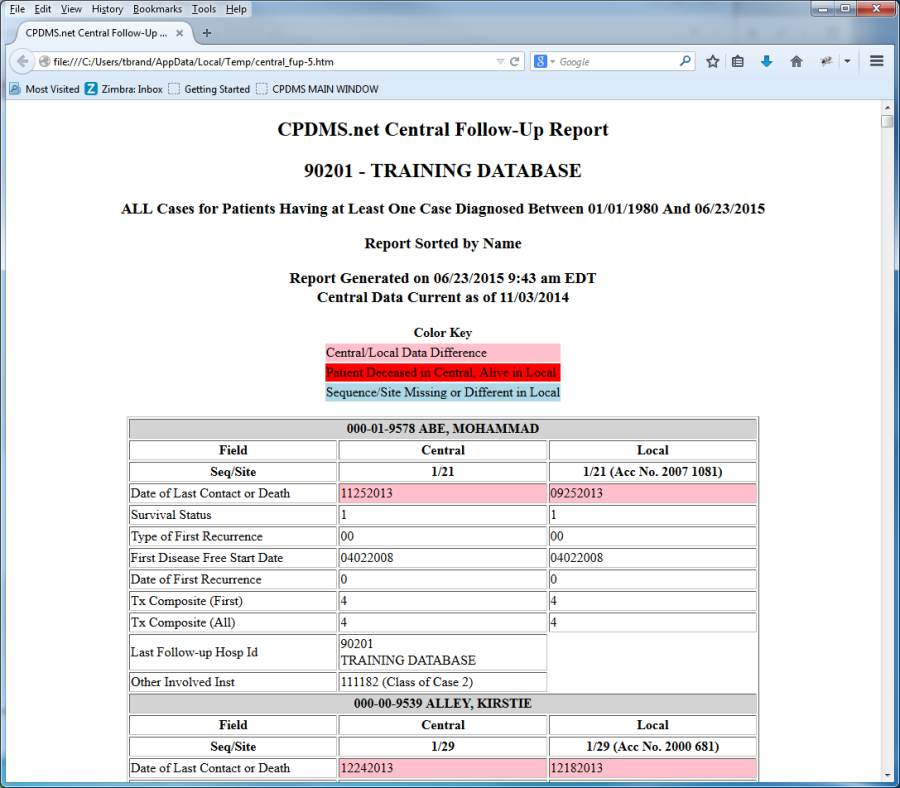
The report lists the facility ID number and name, and the date and sorting parameters which were chosen. Each patient is listed with the values from the central database (on the left) and the local registry database (on the right) for the fields Date Last Contact, Survival Status, Type of First Recurrence, Disease Free Start Date, Date of First Recurrence, Treatment Composite First, and Treatment Composite All. Any difference between the values in central versus local is highlighted in pink, with the exception of discrepancies in Survival Status, which are in red. If a user has chosen to include subsequent record sequences which are in central but not in the local database, these will be listed and highlighted in blue. The ID number and name of the institution which was the source of the data in central is listed, as well as the ID number and class of case of any other facilities associated with that record.